Focus on Africa: What Foreign Aid Data Says About the Continent’s— and the World’s — COVID Response

As COVID-19 wears on, more data emerges about the pandemic response. Cooper/Smith’s mission is to make this data accessible to policymakers and people working in health systems, so they can use it to make better decisions.
Today, policymakers face pressing questions about how to allocate foreign aid for COVID-19. Is it going to the right places? How can we tell who needs more?
We created a set of simple dashboards to help answer those questions. The dashboards use Tableau Public to display a range of financial and epidemiological data.

These data contain an inherent limitation: the extremely low level of testing across Africa. That makes it hard to assess the scale of each African country’s COVID challenge and to draw comparisons across the continent.
In high- and many middle-income countries, testing has been robust enough to use reported case counts as a fair representation of the state of the epidemic in a given country. Africa, however, is running far fewer tests: about 25 times fewer per capita than North America or Europe.
With so little testing in most African countries, we can’t simply rely on COVID cases or COVID deaths per capita to assess the severity of a country’s epidemic or its capability to respond.
Is aid being matched to greatest need?
Because case counts are unreliable, we looked for other metrics that can help help find possible mismatches between need and level of COVID aid.
A caution: How much aid a country needs is an irreducibly complex question, and many factors are difficult to measure. It’s also important to avoid a common fallacy: interpreting successful outcomes as evidence that aid isn’t needed. (The success might well be unattainable without the aid.)
The upshot is that the comparisons that follow are a starting point for further investigation into the conditions in a given country, rather than a basis for definitive conclusions. Still, they’re a useful starting point given the available data.
First Possible Proxy: COVID Tests Per Capita
The first possible proxy for need we considered was COVID tests per capita. A country’s level of testing could be a proxy for its ability to mount a strong COVID response.
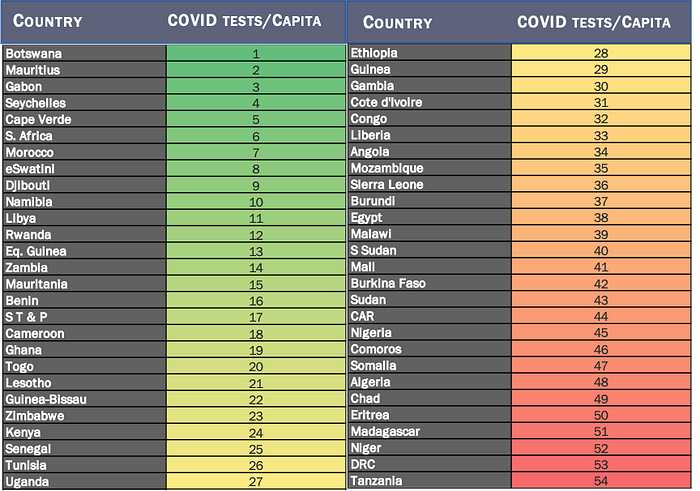
We ranked COVID tests per capita across 54 countries, with dark green indicating the highest level (Botswana), and dark red indicating the lowest levels (Tanzania and DRC).
When discussing Africa and COVID-19 testing, however, it’s important to remember that every country on this list is testing far less than wealthy countries. Even the best performing country — Botswana — is testing only around half as much as North America or Europe. On average, the continent is testing 25 times less, and the worst performing countries are testing up to 500 times less.
Next, we juxtaposed COVID tests per capita with COVID aid per capita. Again, dark green represents the highest level of aid per capita (South Sudan) and dark red represents the lowest level (Angola).

What stands out?
- South Sudan, Central African Republic (CAR), and Zimbabwe are receiving the greatest amount of COVID aid per capita. South Sudan and CAR are both in the bottom 20% of African nations in terms of COVID testing per capita, and likely are in great need of the assistance.
- Zimbabwe is in the middle of the distribution in terms of COVID tests per capita and has received a relatively high level of aid.
- Angola, Benin, and Togo are each receiving very low levels of COVID aid per capita. Yet while Angola is doing poorly in terms of testing, Benin and Togo are in the second-highest quintile.
- A few countries appear to be responding well without aid. Cape Verde, Seychelles, and Mauritius are each doing very well, relatively, in terms of testing, despite not currently receiving COVID-19 aid.
- Some countries receiving middling levels of aid are struggling with testing. Examples include DRC, Niger, Madagascar, and Nigeria.
Finally, some countries continue to struggle on testing despite ranking relatively high in terms of COVID aid per capita. These include South Sudan, Sudan, Somalia, Chad, and Burkina Faso. One likely reason for this is that they entered the COVID crisis with very low levels of baseline health expenditure.
Second Possible Proxy: Total Health Expenditure per Capita
That brings us to a second metric that can help us assess a country’s need for COVID aid: Total Health Expenditure (THE) per capita. Total Health Expenditure is a reasonable proxy for a country’s baseline capacity to provide health services.

What stands out?
- In the previous comparison, Angola appeared to be potentially underfunded relative to its testing level. Inspecting Angola’s THE per capita, however, shows that it spends relatively highly on health, and may therefore be less in need of COVID-specific aid than other African countries.
- Conversely, we see that Benin is spending very little on health, and is still receiving little in terms of aid. While it appeared to be testing in the highest third of African nations, it may generally be in need of help for auxiliary health services and social services supplanted by COVID-19.
- CAR, South Sudan, and Zimbabwe are receiving the greatest amount in terms of per capita COVID-specific aid. However, they are around the median in terms of total health expenditure. Other nations such as Madagascar, Ethiopia, DRC, and Burundi are at the bottom of the distribution for THE, and are likely to need even greater assistance in the COVID-19 era.
Conclusion
These metrics don’t provide definitive answers. Each country has its own distinctive circumstances: the baseline capacity of its health system, the age of its population, economic strength, scientific and laboratory capacity, demographics, and many more.
But these data can help us ask incisive questions. Why, for example, do some West African countries appear to be testing well despite relatively low levels of baseline health spending and COVID aid? These answers, in turn, can help us discover best practices and address unmet needs.
The COVID-19 testing data used for 17 of 54 countries is drawn from Our World in Data, while the remainder is gathered manually from Ministry of Health websites, public data dashboards, and other public sources. Financial data is drawn from a variety of sources, listed on the Data Sources page on our COVID-19 Foreign Assistance website. For questions about our analysis, contact contact@coopersmith.org.
